
Did you know that between 30-50% of moms report some loss of bladder control by age 40, and 65% notice it for the first time either during or after childbirth?
Or that 25% of women notice some change in sexual function persisting beyond 6-months postpartum?
Or that, over time, they can lead to major surgery for at least 11% of women?
These are problems that can diminish quality of life at home, in the bedroom, or at work.
Time to take control of your body. Start with a better understanding of what’s going on down there as you age or give birth.
Pelvic Floor
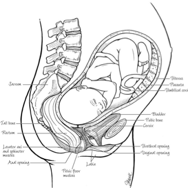
The pelvic floor is a group of supportive muscles and connective tissues that keeps your pelvic organs (uterus, bladder, bowels) in their proper positions. It spans like a supportive shelf from your pubic bone to tailbone, and side-to-side across the bottom of your pelvis.
A strong and healthy pelvic floor helps you maintain control over your bladder and bowels, and helps you to feel normal tone in the vagina.
Your pelvic floor muscles are in a hidden part of your body, but play a critical role by:
- contracting when you cough, sneeze or strain, helping to prevent the accidental leakage of urine.
- helping to hold the pelvic organs (including bladder) in the right position.
- helping in the control of passing of urine, gas and bowel motions.
- playing a role in sexual function during intercourse.
Like any other muscle throughout your body, the pelvic floor muscles need the right exercise, on a regular basis, to be strong and fit!
Pelvic Floor During & After Childbirth
Even during a ‘normal’ pregnancy and delivery, the pelvic floor muscles, connective tissues, organs and nerves undergo tremendous strain and become stretched and weakened.
Even when external signs of injury aren’t present, it’s been shown that the vast majority of women have injury to the deeper muscles. After childbirth, it’s important to rehabilitate your pelvic floor.
What Happens When the Pelvic Floor is Injured or Weak?
Pelvic Organ Prolapse
The vagina is like a horizontal tube with strong upper and lower walls, with the upper wall providing major support underneath the urethra and bladder, and the lower wall helping to keep the rectum in its proper position. Several ligaments that attach to the bones of the pelvis support the uterus, cervix and upper apex of the vagina.
Under normal conditions, the strength within the vaginal walls, and their attachments to the pelvis, play essential roles in keeping the nearby organs (uterus, bladder, rectum and bowel) where they’re supposed to be.
When prolapse occurs months, years or even decades after childbirth, support might have been lost around one or all of these areas. Different types of prolapse often cause their own distinct symptoms and call for different treatments.
Learn more about how we treat pelvic organ prolapse.
Cystocele: The ‘Dropped Bladder’
A cystocele forms when the upper vaginal wall loses its support, allowing the bladder to drop, sometimes causing a vaginal bulge and/or difficulty emptying the bladder.
Rectocele: The ‘Bulging Rectum’
A rectocele results from bulging of the rectum into a weakened lower vaginal wall, sometimes leading to vaginal bulging and/or difficulty having bowel movements. Some women with rectoceles feel that stools feel like they’re getting ‘stuck’ in the lower part of the rectum.
Uterine Prolapse
This occurs when the uterus and cervix drop down toward the opening of the vagina after the ligaments supporting them have weakened. It may cause pressure sensations in the vagina, rectum or even lower back.
Perineal Injury
The perineum is the skin and muscle spanning between the vaginal and anal openings. It has a lot of nerve endings and plays an important role in helping you feel normal tone in the vagina and during intercourse.
The perineum very often injured during vaginal childbirth, due to natural stretching and/or episiotomy. After these injuries, some women complain of feeling ‘too loose’ and others complain of pain or tenderness.
Stress Urinary Incontinence
Stress incontinence (“SUI”) is leakage that occurs at the moment of a cough, sneeze, exercise or other physical stress.
Studies have found that for women between ages 30-45, vaginal childbirth carries a two- to five-times higher risk of having SUI.
If you’ve developed SUI during or after childbirth, one particular anatomical change is the most common culprit: weakening of the vaginal wall that lies beneath the urethra and provides its main support. This is called urethral hypermobility.
If you have stress incontinence after childbirth, you like worry it be permanent. In many cases, the problem will resolve as the tissues naturally heal; but one study found that if SUI is still present 3 months after delivery, there are 94% odds that it will not spontaneously resolve.
But don’t worry! With pelvic strengthening many cases improve; and if not, there are simple ways (for instance: the sling procedure) to completely eliminate SUI for over 90% of women.
Overactive Bladder (OAB)
Do you map the next bathroom when you’re out of the house, anticipating the next sudden urge? If so, you may have OAB.
This condition causes strong urges to urinate, frequent trips to the bathroom during the day and sometimes night, and sometimes leakage before reaching the bathroom
Around 30% of childbearing women have this condition, and one study estimated that 80% of affected individuals are not receiving treatment. Research done right here at Women’s Pelvic Surgery Specialists has proven that OAB symptoms become more common after each pregnancy and childbirth. The condition is very treatable with changes to your diet and bladder behavior, as well as medications and other non-surgical options.
Anal Incontinence & Bowel Problems
Diminished control over the bowels (whether stool or gas) is one of the most distressing and embarrassing problems faced by post-reproductive women. By age 45, it’s 8 times more prevalent in women than men, occurring in around 25% of women who have had a previous vaginal delivery. Sometimes this is due to injury to the anal sphincter muscles.
An article from 1993, in The New England Journal of Medicine showed that hidden injury to the sphincter occurs in up to 34% of ‘normal’ appearing deliveries, and up to 44% in women after 2 or more vaginal births.
The good news? We find the majority of cases will be controlled with changes to diet and fiber, over-the-counter supplements and other non-surgical strategies.
Sexual Dysfunction
Sexual disorders have been reported in approximately 14% of women after routine vaginal delivery, and the risk is thought to be even higher after a forceps or difficult delivery.
This may include a simple change in sexual energy or desire (libido), a diminished physical response (arousal), an inability to reach orgasm (anorgasmia), or perhaps even physical pain during intercourse (dyspareunia).
As a new mom, if you’re experiencing problems and you think they’re not just due to the exhaustion and new pressures that can impact your sex life, you should consider having a physical assessment of your perineal and pelvic floor healing.
Common post-childbirth issues may include:
- A sore or incompletely healed perineum
- Lack of estrogen leading to dryness and pain. Sometimes this lack of estrogen is the result of breastfeeding, which has strong hormonal effects.
- Body image concerns as some body changes after childbirth are short-term, and others may be long-term.
Diastasis (Injury to the Abdominal Muscles) and Cosmetic Issues
Although physical changes in the pelvic and vaginal area are best addressed by urogynecologists, other specialists are available to address changes to ‘body after baby’ changes that occur outside the pelvic floor.
Diastasis (separation of the abdominal muscles) occasionally occurs after childbirth and can cause significant discomfort and dysfunction. The symptoms associated with this condition sometime improve with the help of a physical therapist, and in other cases will not improve without surgery.
Women’s Pelvic Surgery Specialists is available for consultation for diastasis or any other cosmetic issues of significant concern.
5 Questions to Decide Whether You Need Help
After learning more about the pelvic floor, and common concerns women have about their pelvic floor health, you may be wondering if you could benefit from the expertise we offer at Women’s Pelvic Surgery Specialists.
Start with our quick five question assessment.
- Can you strongly contract your pelvic muscles for 10 seconds?
- Do you have pain in the pelvis, bladder, rectum or vagina?
- Have you experienced a loss of bladder function?
- Have you experienced a loss of bowel function, or constipation?
- Have you noticed a change “down there” that impacts your self confidence, comfort or control?
Then, contact us to see how we can help.
Adapted from “Ever Since I Had My Baby” by Roger Goldberg; Penguin Random House https://www.penguinrandomhouse.com/books/61217/ever-since-i-had-my-baby-by-roger-goldberg-md-mph/